Intussusception is a condition commonly encountered in young children but is often overlooked in its early stages due to nonspecific symptoms that can be easily mistaken for gastrointestinal disturbances. Early recognition of warning signs and associated risk factors enables parents to seek timely hospital care, thereby increasing the likelihood of successful non-surgical management and reducing the risk of serious complications.
What is intussusception? Which age groups are most susceptible to intussusception?
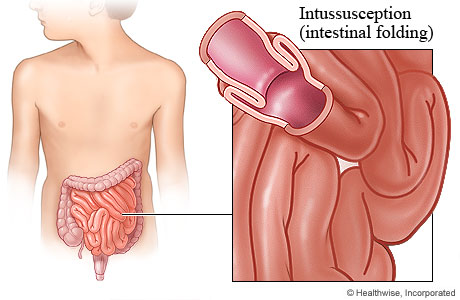
What is intussusception?
Intussusception is a condition in which one segment of the intestine telescopes into the lumen of an adjacent intestinal segment, resulting in partial or complete bowel obstruction. When this occurs, the mesenteric blood supply to the affected bowel is compromised, leading to rapid ischemia, edema, inflammation, and, if not managed promptly, progression to bowel necrosis and perforation.
Intussusception is one of the leading causes of intestinal obstruction in children and is particularly dangerous due to its rapid progression and the limited ability of young children to clearly articulate their symptoms.
Which age groups are most susceptible to intussusception?
Intussusception can occur at any age but is most commonly seen in children between 6 months and 3 years of age. Approximately 65% of cases occur before the age of one, and 80–90% are diagnosed before two years of age, a period during which intestinal motility is not yet fully mature.
Causes of intussusception
At present, the exact cause of intussusception in most young children remains unclear. However, several factors have been identified as being associated with an increased risk of developing the condition, including:
- Weaning period: Dietary changes during the weaning phase may increase intestinal peristalsis, predisposing to dysregulated bowel contractions.
- Discrepancy in intestinal segment size in infants: When a larger bowel segment invaginates into a smaller one, the risk of intussusception increases.
- Mesenteric lymphadenitis, enteritis, or intestinal adhesions: Inflammatory conditions may disrupt normal peristalsis and create a pathological “lead point” for intussusception.
- Recent respiratory viral or gastrointestinal infections: Intussusception frequently occurs following viral illnesses that induce abnormal intestinal motility.
- Infants aged 3–6 months, male sex, and well-nourished infants: These populations are considered at highest risk and require close monitoring.
- Congenital gastrointestinal anomalies: A significant risk factor, particularly in older children.
- History of intussusception or family predisposition: Children with a prior episode have an increased risk of recurrence.
- Immunodeficiency: Associated with higher susceptibility to infections and gastrointestinal dysfunction.
- Seasonal pattern: The condition is more commonly observed during autumn and winter, coinciding with peaks in viral infections.
- In older children: Intussusception is more likely to be associated with an identifiable organic cause, such as Meckel’s diverticulum, intestinal polyps, enteric duplication cysts, or benign and malignant tumors of the small intestine.
Symptoms of intussusception that parents should pay close attention to
The clinical manifestations of intussusception progress rapidly and intensify over time, and are typically classified into the following stages:
Early-stage symptoms of intussusception that are easily overlooked
- A child who is feeding and playing normally may suddenly cry inconsolably, refuse feeding, or stop playing. This is an early but easily misinterpreted sign, often mistaken for common irritability.
- Paroxysmal crying accompanied by drawing the knees toward the chest or arching of the body due to abdominal pain, resulting from intestinal spasms as the bowel telescopes.
- Vomiting of food contents or green or yellow fluid, indicating the early onset of intestinal obstruction.
- Cold sweats with the pallor of the skin.
- A key clinical feature is that the pain occurs in intermittent episodes, typically every 15 to 20 minutes. Between episodes, the child may appear temporarily calm or even resume feeding, which often leads caregivers to underestimate the severity of the condition.
Severe-stage symptoms of intussusception
- Children may pass stools mixed with mucus and blood or fresh blood.
- Marked fatigue and lethargy with signs of dehydration, including dry lips.
- Fever accompanied by cold extremities and pale skin.
- A palpable abdominal mass corresponding to the intussuscepted bowel segment may be detected on physical examination.
Late-stage, life-threatening symptoms of intussusception
- Persistent vomiting with progressive abdominal distension.
- Cold, pale skin with rapid, shallow breathing.
- Weak, rapid pulse, altered mental status, lethargy, or coma.
- Signs of severe dehydration, systemic infection, and septic shock.
Parental note: Not all children present with the full spectrum of symptoms. Therefore, parents should seek immediate medical evaluation whenever any abnormal signs are observed to allow for timely assessment and early diagnosis.
Diagnosis of intussusception
Because affected children are typically very young, diagnosis relies primarily on the clinical presentation in combination with paraclinical investigations, including:
- Abdominal ultrasonography, which is the preferred first-line modality due to its noninvasive nature and high diagnostic accuracy.
- Plain abdominal radiography, which assists in evaluating the presence of intestinal obstruction and associated complications.
- Abdominal computed tomography (CT), which is reserved for diagnostically challenging cases or when complications are suspected.
How is intussusception treated?
Pneumatic reduction of intussusception under DSA guidance
This is a modern therapeutic approach for pediatric intussusception, in which air or contrast fluid is insufflated into the colon via a rectal catheter under continuous monitoring with a digital subtraction angiography (DSA) X-ray system. By precisely controlling intraluminal pressure and the direction of reduction, the intussuscepted bowel segment can often be reduced spontaneously without the need for surgery. This technique offers high efficacy, is minimally invasive, and ensures a high level of safety for pediatric patients.
Currently, pneumatic reduction of intussusception under DSA guidance is routinely performed at Hong Ngoc General Hospital by Specialist Level I Physician Bach Phuc Huy, Deputy Head of the Department of General Surgery. The technique has enabled many children to be treated safely without surgical intervention, facilitating rapid recovery and minimizing the risk of complications.
For detailed consultation, please contact the hotline at 0949 646 556.

Surgical reduction of intussusception
In cases where the child presents late or when pneumatic or hydrostatic reduction is unsuccessful, surgical intervention is indicated to reduce the intussusception. Depending on the extent of bowel injury, the procedure may involve bowel resection with anastomosis or the creation of a temporary stoma, along with antibiotic therapy when concomitant infection is present.
Bowel resection
In very late-presenting cases where intestinal necrosis has occurred, surgical resection of the affected bowel segment is mandatory to control complications. However, postoperative resuscitation and care are complex, and the child faces a high risk of serious complications, including malnutrition, infection, and pneumonia.
Where is pediatric intussusception treated? A trusted 24/7 emergency center for intussusception
The Gastrointestinal Surgery Unit at Hong Ngoc General Hospital operates a 24/7 emergency protocol for the management and treatment of pediatric intussusception. Early and timely intervention enables many children to undergo safe non-surgical reduction, significantly reducing the risk of bowel necrosis and other serious complications.
- Highly specialized medical team: Direct examination and intervention are performed by Specialist Level I Physician Bach Phuc Huy, Deputy Head of the Department of General Surgery, with more than 15 years of experience in gastrointestinal surgery.
- Advanced technology and techniques: Pneumatic reduction of intussusception using digital subtraction angiography (DSA), a minimally invasive approach that reduces pain, shortens treatment duration, and facilitates rapid recovery.
- Modern operating theaters and internationally standardized safety protocols: Accredited with global surgical certification from the Royal College of Surgeons (RCS) of England and international healthcare quality certification from the Australian Council on Healthcare Standards International (ACHSI).
- Standardized inpatient care: Clean, well-equipped patient rooms with nursing staff available 24/7.
- Comprehensive insurance coverage: Acceptance of national health insurance and private health insurance plans.

Note: The information provided in this article by Hong Ngoc General Hospital is for reference purposes only and does not replace professional medical diagnosis or treatment. For an accurate assessment of the condition, patients should visit a reputable healthcare facility for direct evaluation and consultation with a qualified physician regarding an appropriate treatment plan.
Center for Gastroenterology and Colorectal–Perineal Disorders
- Hong Ngoc Phuc Truong Minh General Hospital - No. 8 Chau Van Liem Street, Nam Tu Liem District, Hanoi
- Hong Ngoc General Hospital55 Yen Ninh Street, Ba Dinh District, Hanoi
- Hotline: 0911 908 856 – 0932 232 016
Email: trungtamtieuhoa@hongngochospital.vn
Follow the official fanpage of the Center for Gastroenterology – Hong Ngoc General Hospital for additional useful health information.